AC Joint Dislocation
The shoulder is the most mobile joint in the body, it requires a complex system of structures to keep it stable during movement. Because it supports the shoulder and the scapula, the clavicle (collar bone) is an important aspect of shoulder stability and function (shoulder blade). The clavicle and the acromion, a component of the scapula, create a joint. The Acromioclavicular Joint (ACJ) is a tiny joint that allows extremely modest motions between the scapula and clavicle during normal shoulder motion. Unfortunately, this joint is vulnerable to injury.
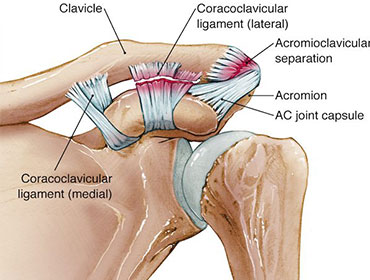
The ACJ is stabilised by a complicated ligament structure. The acromioclavicular capsular ligaments and the Coroclavicular (CC) ligaments, which are made up of the coronoid and trapezoid ligaments, can be split into two groups. An Acromioclavicular Joint (ACJ) dislocation or separation can occur when these ligaments are damaged.
When the clavicle dislocates from the acromion, it is known as an ACJ dislocation or separation. Different degrees of injury can develop depending on the severity of the injury, ranging from Grade I to Grade VI. The more severe the injury, the more conspicuous the clavicle becomes displaced. Surgical intervention is usually not required for Grades I–II, but it is required for Grades IV–VI. Grade III injuries may necessitate surgery, although the decision to do so is largely based on the patient's symptoms, as well as the individual's needs and, in certain cases, the types of sports and activities they participate in.
Treatments:
The severity of an AC joint dislocation determines how it is treated. Non-operative treatment is available for Grade I–II injuries. Even if there is still a prominence to the distal clavicle, the pain fades after an initial period of discomfort, leaving a perfectly functional shoulder. However, in certain cases, long-term pain might develop, and if this is the case, it is usually due to some type of inherent injury to the cartilage meniscus found within the acromioclavicular joint. In certain cases, an arthroscopic ACJ excision may be necessary.
Grade III dislocations can be treated conservatively, but surgery may be required in some cases. In a Grade III dislocation, the need for stabilisation surgery is determined by the severity of the symptoms and, more importantly, the patient's expectations. Athletes and above workers frequently require surgery. Grade IV–VI injuries frequently necessitate surgery to restore shoulder function, particularly when the arm is raised to or above shoulder height.